A clinical briefing for referring GPs on the nationally commissioned lung volume reduction service at Guy's and St Thomas' — covering endobronchial valve placement, LVRS, and lung transplant assessment within a single monthly specialist MDT.
Last reviewed: April 2026 · Dr Lawrence Okiror FRCS(CTh) FRCSEd(CTh) · GMC 6150382
Nationally commissioned Advanced Emphysema Surgical Service at Guy's and St Thomas'. Endobronchial valve therapy, LVRS, and transplant assessment for appropriate patients.
Patient selection
Patients require severe emphysema (FEV1 15–50% predicted), significant hyperinflation (RV >150%), and must have completed pulmonary rehabilitation. Low homogeneous disease may be suitable for valves.
Referral
Contact Jo Mitchelson on 020 7952 2882 for pre-assessment guidance. Patients who meet NICE criteria are referred into the MDT pathway at GSTT. Private assessment available within 2–3 days.
The Case for Assessment
Beyond Medical Optimisation
For patients with severe emphysema who remain symptomatic on maximal inhaled therapy and have completed pulmonary rehabilitation, the clinical assumption is often that nothing further can be offered. In many cases this assumption is wrong. A spectrum of interventional and surgical options exists — endobronchial valve placement, lung volume reduction surgery, and lung transplant assessment — that can produce meaningful improvements in breathlessness, exercise tolerance, and quality of life in appropriately selected patients. The critical step is a comprehensive specialist assessment.
Nationally Commissioned
Guy's and St Thomas' NHS Foundation Trust holds NHS England national commissioning for both LVRS and endobronchial valve placement — one of a small number of designated centres in England.
100+ Interventions
Combined EBV and LVRS procedures performed since Mr Okiror's appointment in February 2019 — the sole operator for both procedures at GSTT and London Bridge Hospital.
All Four Options
The monthly specialist MDT considers EBV, LVRS, lung transplant assessment, and continued medical optimisation for every referred patient. No pathway is predetermined before the MDT discussion.
Private assessment is available within 2–3 working days, with the full workup — spirometry, HRCT review, Chartis collateral ventilation assessment, V/Q SPECT-CT, and MDT discussion — typically completed within a few weeks. NHS waiting times for intervention are approximately 4–6 months. For a patient with declining FEV1 and contracting exercise tolerance, that interval carries functional consequences that are not always recoverable.
Patient Selection
Which Patients to Refer
Intervention is not appropriate for all COPD patients — but the eligible population is larger than is commonly recognised. The MDT assessment determines which, if any, intervention is appropriate. GPs should refer for assessment, not for a specific procedure.
→
GOLD stage III–IV on maximal inhaled therapy with completed pulmonary rehabilitation
→
Upper lobe predominant emphysema on CT with significant hyperinflation (RV >150%, TLC >100%)
Non-smoker or confirmed smoking cessation; BMI <35; no significant active infection or bronchiectasis
→
Any patient who has been told no further treatment options are available and has not had a formal LVR assessment
V/Q SPECT-CT scanning provides functional heterogeneity mapping to guide target lobe selection. A nuclear medicine physician with specific expertise in emphysema functional imaging attends every MDT. Patients do not need to be surgical candidates at the point of referral — the MDT will determine what is appropriate.
The Procedure in Practice
Endobronchial Valves Deployed Bronchoscopically
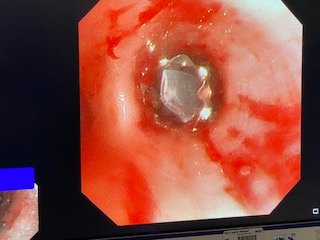
Intraoperative bronchoscopic images from Mr Okiror's own clinical practice, showing endobronchial valves immediately following deployment. The valve creates a one-way seal in the target airway, allowing air to escape from the diseased lobe on exhalation while preventing re-entry — causing progressive deflation of the hyperinflated tissue.
Endobronchial valve in situ immediately following bronchoscopic deployment. The valve is visible at the target airway orifice.
Bronchoscopic view showing the deployed valve. The procedure requires no surgical incision and is performed under general anaesthesia.
The Specialist MDT
All Four Options On the Table
A monthly specialist MDT at GSTT considers every referred patient. The MDT includes respiratory physicians, a COPD clinical nurse specialist, thoracic radiologist, nuclear medicine physician, and — uniquely — a lung transplantation physician and surgeon from Harefield Hospital. This means all four management options are evaluated within the same discussion.
1
Endobronchial Valve Placement (EBV)
Bronchoscopic lobar occlusion under general anaesthesia. Candidacy is determined by Chartis collateral ventilation assessment and fissure completeness on HRCT. NICE-recommended (TA457) and supported by the LIBERATE RCT (NEJM, 2018), which demonstrated significant improvements in FEV1, six-minute walk distance, and quality of life at 12 months versus medical management. Inpatient stay 2–3 days for monitoring and management of the risk of post-procedural pneumothorax. Fully reversible — valves can be removed bronchoscopically.
2
Lung Volume Reduction Surgery (LVRS)
Surgical resection of the most destroyed emphysematous tissue, typically upper lobe predominant. Performed robotically or by VATS — no thoracotomy. Indicated where collateral ventilation precludes EBV, or where surgical heterogeneity is greater. Supported by the CELEB trial (Lancet, 2019) — the UK's direct RCT comparison of LVRS versus EBV — confirming both procedures are effective in appropriately selected phenotypes, with patient-level selection determining relative benefit. GSTT holds NHS England national commissioning for both LVRS and EBV.
3
Lung Transplant Assessment
A lung transplantation physician and surgeon from Harefield Hospital attend every MDT. Where transplant candidacy is relevant — whether as primary management or as the next step after failed EBV or LVRS — that assessment begins within the same MDT discussion, not after a separate onward referral. For patients where disease severity and functional trajectory make transplant listing the most appropriate recommendation, the pathway is already open.
4
Continued Medical Optimisation
Not every patient assessed will proceed to intervention. For those who do not meet selection criteria or choose not to proceed, the MDT provides a comprehensive review of medical management — inhaler optimisation against current GOLD guidance, pulmonary rehabilitation pathway, long-term oxygen assessment, and breathlessness management. A detailed MDT letter is sent to the referring clinician regardless of outcome, including the rationale for any decision not to intervene.
Make a Referral
How to Refer
Patients can be referred directly for MDT assessment without specifying a preferred intervention. A brief referral letter with recent spirometry, CT chest report, and current inhaler therapy is sufficient. Private assessments are available within 2–3 working days, with the full workup and MDT presentation typically completed within weeks. No GP referral letter is required for private assessment; patients may also self-refer.
AXA · BUPA · WPA · Vitality · Cigna · Aviva · and other major insurers · Self-pay
Download & Further Reading
The full GP clinical briefing document covers the complete evidence base, patient selection criteria, MDT composition, private and NHS pathway comparison, and referral contact details.